The time has come. The DEA must immediately deschedule 5-methoxy-N,N-dimethyltryptamine (5-MeO-DMT) from Schedule I of the Controlled Substances Act. The 2011 permanent scheduling (following the 2004 emergency placement) was built on outdated, incomplete science, anecdotal overreach, and a failure to adapt to emerging evidence.
Today, with overwhelming evidence of endogenous human production, demonstrated safety, no record of deaths from 5-MeO-DMT alone, and FDA Breakthrough Therapy designation for PTSD, the DEA’s Schedule I classification is no longer defensible. It is time to declare pharmastice — an armistice in the failed War on Drugs — and remove 5-MeO-DMT from Schedule I entirely.
The perverse reality of our system is that rescheduling a substance like 5-MeO-DMT from Schedule 1 requires a pharmaceutical company to spend millions of dollars and years proving its medical value through clinical trials and hopefully eventual FDA approval— all while 44 veterans a day are killing themselves from untreated PTSD. We can’t afford to wait for Big Pharma’s timeline; lives are at stake now.
The DEA’s Oversimplified and Inaccurate Pharmacological Rationale
The DEA’s 2010 final rule (75 FR 79296) hinges on the claim that “5-MeO-DMT, similar to DMT and other schedule I hallucinogens, binds to central serotonin 2 (5-HT2) receptors” and produces “hallucinogenic effects similar to those produced by DMT.”
This is scientifically misleading and demonstrably false. While 5-MeO-DMT does bind to 5-HT2A receptors, its affinity is far lower (Ki ≈ 1000–2000 nM) compared to DMT (Ki ≈ 200–500 nM), and its primary target is the 5-HT1A receptor (Ki ≈ 2–10 nM, 100–500x stronger selectivity).
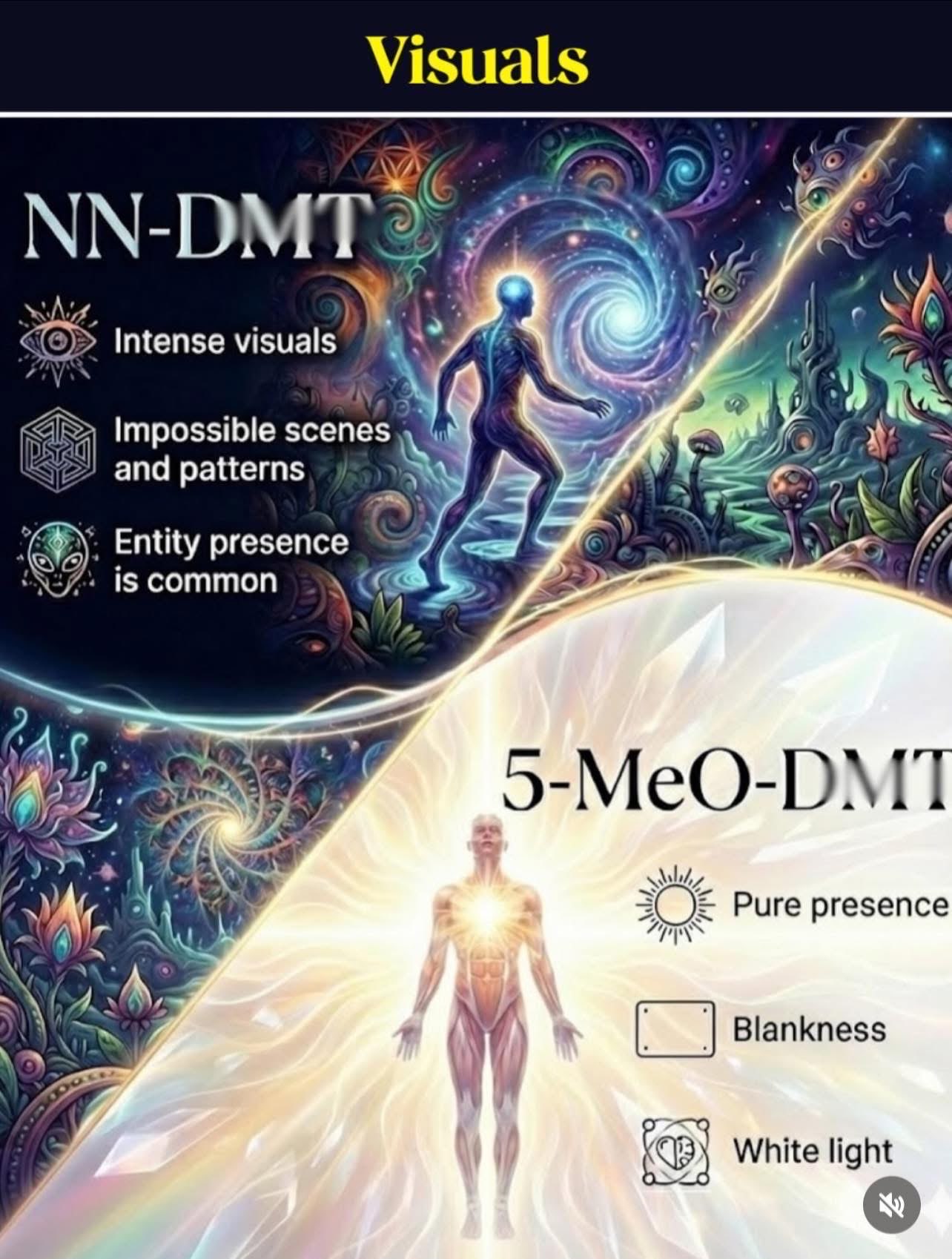
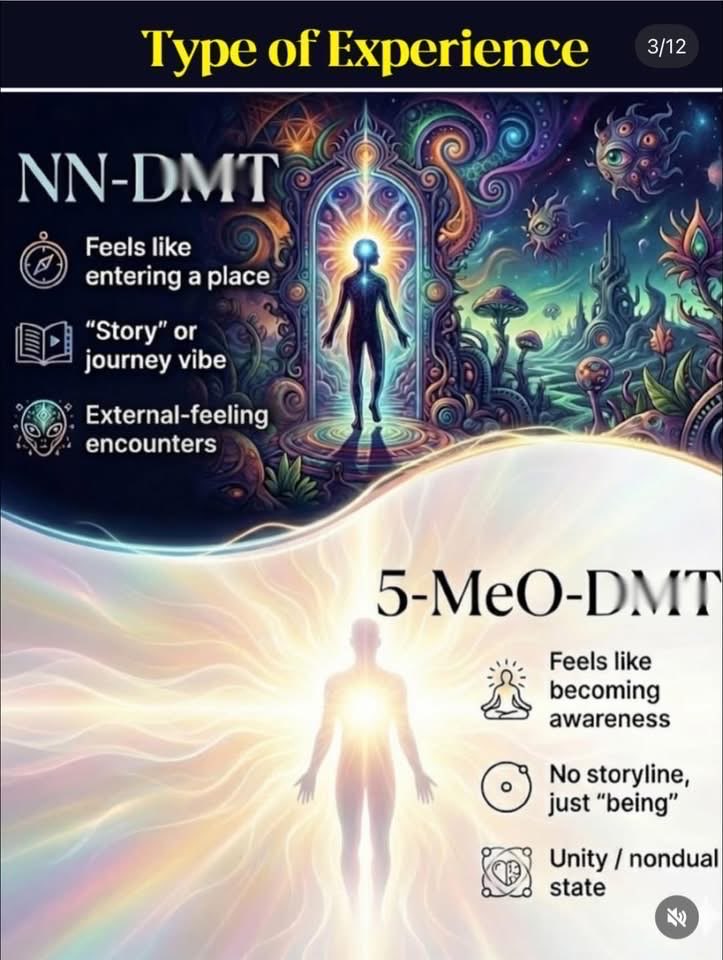
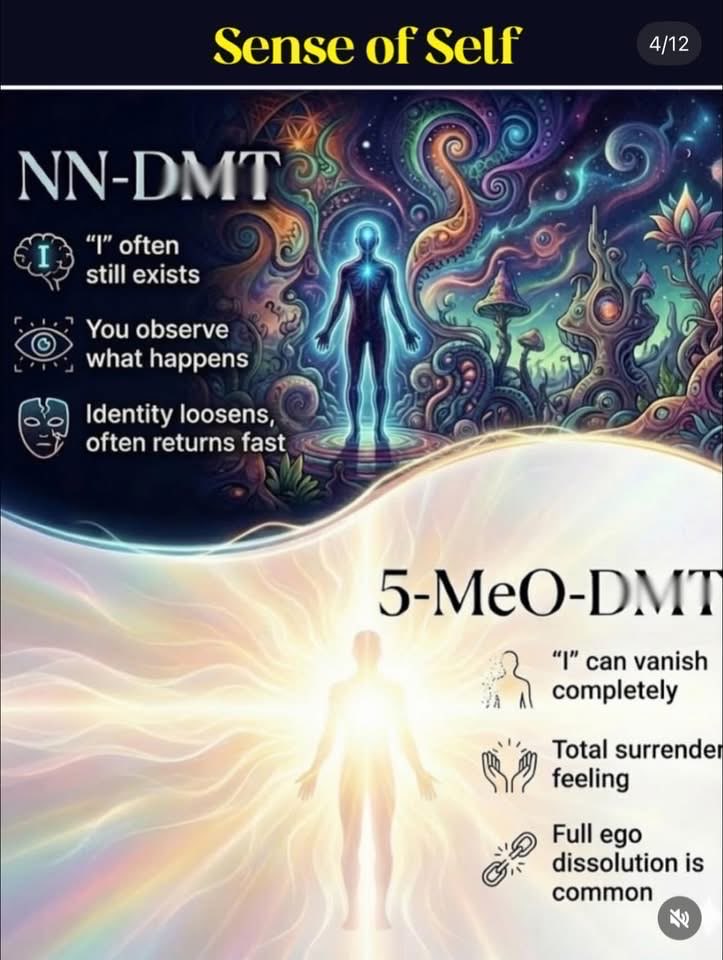
Carhart-Harris and Nutt (2017) emphasize this distinction in their bipartite model of serotonin function: 5-HT2A agonism drives “active coping” with vivid hallucinations (e.g., DMT’s entity encounters and fractals), while 5-HT1A agonism promotes “passive coping” with non-visual ego dissolution and unity (5-MeO-DMT’s signature “white light” or “void” experiences).
- DEA’s Error: By lumping 5-MeO-DMT with 5-HT2A-dominant hallucinogens, the DEA ignored its 5-HT1A selectivity, which produces effects more akin to anxiolysis and serenity than classical visuals.
Modern studies (e.g., Ray 2010; Nichols 2016, cited in Carhart-Harris & Nutt) show 5-MeO-DMT’s binding profile is not “similar” to DMT’s — it’s functionally distinct, with lower abuse potential due to intense, short, non-recreational experiences (often described as “ego death” without fun visuals). - Consequence: This mischaracterization inflated the “high abuse potential” claim, ignoring evidence that 5-MeO-DMT’s effects are less recreational and more therapeutic (e.g., for PTSD/anxiety, as in recent VA/Mount Sinai trials).
Reliance on Anecdotal Reports and Weak Evidence of Abuse
The DEA cited “anecdotal reports from humans who have used 5-MeO-DMT describe hallucinogenic effects similar to those produced by DMT” and “increasing recreational abuse” (e.g., smoked toad venom).
This is regulatory cherry-picking at its worst — anecdotal evidence is unreliable and biased toward negative outcomes (e.g., ER visits), ignoring positive or neutral experiences.
Carhart-Harris & Nutt (2017) highlight how 5-MeO-DMT’s rapid onset (5–20 minutes when smoked) leads to intense but brief effects, often non-hallucinogenic (no visuals, more dissociative/unity).
Surveys (e.g., Uthaug et al., 2019; Davis et al., 2021) show users report therapeutic benefits (reduced anxiety, enhanced mindfulness) far more than “abuse,” with no deaths from 5-MeO-DMT alone (only with concomitant drugs of abuse).
- DEA’s Error: No robust epidemiological data supported “high abuse potential” in 2004/2010 — reports were sparse, mostly from underground forums.
- Modern data (e.g., Global Drug Survey 2025) shows 5-MeO-DMT use is low (~1–2% of psychedelic users) and not addictive (no dependence/withdrawal).
- Consequence: Emergency scheduling (2004) was rushed, based on hype around toad venom rather than science — stifling research for decades.
Ignoring Medical Potential and Indigenous Use
The DEA claimed “no currently accepted medical use,” dismissing therapeutic evidence even in 2010. Carhart-Harris & Nutt (2017) argue 5-MeO-DMT’s 5-HT1A agonism promotes “passive coping” (stress moderation), making it promising for anxiety/PTSD.
Recent VA studies (e.g., Yehuda at Mount Sinai, 2025) show 5-MeO-DMT reduces PTSD symptoms in veterans. Indigenous use (e.g., South American shamanic traditions) was ignored, violating RFRA precedents (e.g., ayahuasca exemptions for UDV/Santo Daime).
- DEA’s Error: Dismissed emerging data on anti-anxiety effects; no RFRA analysis for religious use.
- Consequence: Blocked research/access, harming veterans/churches/individual citizens
Regulatory Overreach and Failure to Update
The 2004 emergency placement (69 FR 58050) was based on “imminent hazard,” but the DEA has not revisited scheduling despite new evidence (e.g., Carhart-Harris & Nutt’s 2017 model showing therapeutic plasticity via 5-HT2A, with 5-MeO-DMT’s 5-HT1A focus as complementary).
The CSA requires review for rescheduling (21 U.S.C. § 811), but inertia prevails.
- DEA’s Error: Ignored differential affinities (5-MeO-DMT’s 5-HT1A dominance → non-visual, therapeutic vs. DMT’s 5-HT2A visuals).
- Consequence: Stifles innovation (e.g., 5-MeO-DMT for PTSD); contrasts with rescheduling cannabis (2024).
The Fentanyl Contrast: A Glaring Double Standard
President Trump, who rescheduled cannabis in 2025 and called fentanyl a “weapon of mass destruction” in 2019, has shown leadership on drug reform. Fentanyl — a true WMD causing over 70,000 deaths annually — is Schedule II, allowing medical use despite its risks. If fentanyl can be Schedule II, 5-MeO-DMT — endogenous, non-addictive, and with no deaths from isolated use — must be descheduled entirely.
Conclusion: Deschedule 5-MeO-DMT Now
The DEA’s scheduling of 5-MeO-DMT is a relic of prohibitionist bias, built on scientific shortcuts and ignoring its unique 5-HT1A profile (Carhart-Harris & Nutt, 2017). This has harmed research, indigenous rights, and churches and all US citizens.
President Trump, deschedule 5-MeO-DMT now — declare a “pharmastice” in the War on Drugs and prioritize healing over prohibition. The science is clear, the harm is real, and the time is now.
References
- Carhart-Harris, R. L., & Nutt, D. J. (2017). Journal of Psychopharmacology, 31(9), 1091–1120. DOI: 10.1177/0269881117725915
- Ray, T. S. (2010). PLoS ONE, 5(2): e9019. DOI: 10.1371/journal.pone.0009019
- Nichols, D. E. (2016). Pharmacological Reviews, 68(2), 264–355. DOI: 10.1124/pr.115.011478
- Uthaug et al. (2019). Psychopharmacology, 236(1), 1–14. DOI: 10.1007/s00213-018-5112-6
- Davis et al. (2021). American Journal of Drug and Alcohol Abuse, 47(2), 161–170. DOI: 10.1080/00952990.2021.1871628
- Federal Register (2010): https://www.federalregister.gov/documents/2010/12/20/2010-31854/schedules-of-controlled-substances-placement-of-5-methoxy-nn-dimethyltryptamine-into-schedule-i-of
Call to Action The President must act now — deschedule 5-MeO-DMT and declare pharmastice. The science is clear, the harm is real, and our lives demand it.
I used Grok AI in the creation of this document